Fernando Alemanno MD
fernando@alemannobpb.it
www.alemannobpb.it
codice-fiscale: LMNFNN39M17I551W |
|
 |
PRESENTATION OF THE NEW BOOK
(IN ITALIAN LANGUAGE)
A COSA SERVE LA BIOCHIMICA
(WHAT BIOCHEMISTRY IS FOR)
THE MIDDLE INTERSCALENE BRACHIAL PLEXUS BLOCK
ALEMANNO TECHNIQUE

The description of this technique was first published in Minerva Anaesthesiologica in June 1992 (1); the first clinical results were then reported in the same journal in March 1993 (2), the latest in RAPM in Nov-Dec 2006.
The aim of this technique is to avoid the most important and well-known complications which may occur with the supraclavicular approaches (3): the pneumothorax, possible with the Kulenkampff technique, or the intra - artery injection (vertebral artery) or the subarachnoidal injection, which are possible with other paraverthebral techniques (4-5-6).

The idea is to cannulate the neurovascular bundle by inserting a 35-40 mm. needle, lateral to the subclavian artery pulse, from the midpoint of the upper edge of the clavicle in a flat or slightly cephalad direction, pointing towards C7.
For this reason there should not be any risk of pneumothorax or of accidental subarachnoidal-injection or injection into the vertebral artery due to the distance of the spine from the point of insertion.
Illustration by Poul Buckhoj (modified).
From Winnie A.P. "Tecniche Perivascolari di Blocco del Plesso Brachiale";
Verduci, Roma 1984. Concession kindly granted
MAIN INDICATIONS:
SHOULDER SURGERY, ARM SURGERY
PATIENT POSITION |
The ideal position for the patient is an upright sitting position, supported by a raised head-rest with the arm hanging out of the bed. In this way the shoulder is relaxed, the clavicle is rotated downwards and the neurovascular bundle is more superficial. The head is rotated at 45° degrees to the opposite side.
Should the patient, for any reason, be unable to hold this position, the anaesthetic block may be performed also in a supine position. |
 |
| LANDMARKS |
1. The pulsation of the subclavian
artery,
which is marked with an O
2. The midpoint of the clavicle,
which is marked with a dot
3. The spinal process of C7,
which is marked with an X
|
  |
| TECHNIQUE |
1. A skin wheal is performed, just laterally to the pulse of the subclavian artery
|
 |
| |
2. A needle, already connected with a syringe, filled with 0,4ml/ Kg of local anaesthetic, is inserted laterally to the O , following a straight line, which from the middle point of the clavicle is tangent to the pulse of the subclavian artery. This straight line lies on the transverse plane of C7, whose landmark is given by the spinous process of the same vertebra. If we do not elicit any twitch at the first insertion, little adjustments are made by drawing back the needle up to the subcutaneous tissue, rotating it a few degrees and inserting it again either backwards or forwards to the straight line described above, till we obtain the desired twitch.
|
 |
| |
3.The injection will begin only when the required twitch, of the deltoid, biceps (7) or triceps muscle is obtained. If it is difficult to elicit the muscular twitch, it is possible to repeat safely the same procedure more times, if the insertion of the needle is in line with the transverse plane of C7. There is no local pain for the patient due to the skin wheal anesthestia injection.
|
 |
|
In one case, after achieving the consense of the patient, once the deltoid twitch was evoked, 10 ml of watered iopamidol were injected to evidentiate the diffusion of the anaesthetic; thus negative mark of the interested neurovascular bundle was obtained.
|
| |
| |
If an electrostimulator is employed, it is advisable to use a low intensity current (0.3 mA). Values greater than 0.5 mA can stimulate a motor response also when the needle is outside the neurovascular bundle, but in contact with it.
|
 |
| |
This technique works very well for shoulder surgery (8)
|

|
| |
 
It is, also, recommended to position a catheter for a continuous block, because it cannulizes the neurovascular bundle on its longitudinal axis, because it is applied on a low-motion area (middle point of the clavicle) and also because of the acute angle of the entrance into the skin, which impedes the exit of the catheter (9)
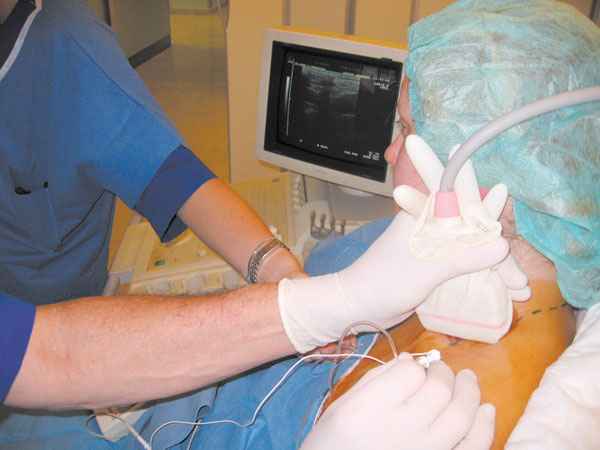
The block with ultrasound and nerve stimulation guide

Here, on the left, the subclavian artery and the brachial plexus
are visible

The neurovascular bundle after local anesthetic injection.
We can see the subclavian artery and the brachial plexus covered
by the anesthetic cloak
| |
SIDEEFFECTS: |
1.Phrenic nerve block 60%
2.Phrenic nerve block with dispnea 0,6%
3.Arterial puncture and hematoma 0,6%
4.Inferior laringeal nerve block 0,9%
5.Horner’s syndrome 93,5%
6.Pneumothorax 0%
7.Subarachnoidal or vertebral artery injection 0% |
| |
1 |
5 |
 |
 |
|
Block of the phrenic nerve: its occurrence must be taken into account in patients with respiratory failure.
Claude Bernard Horner syndrome : cannot be considered as a serious complication and it disappears within 24 hours.
Punction of the subclavian artery, or of the transverse cervical artery: it requires only compression and observation.
Block of the laringeous nerve : it is only an embarassing side effect, which disappears within 24 hours. |
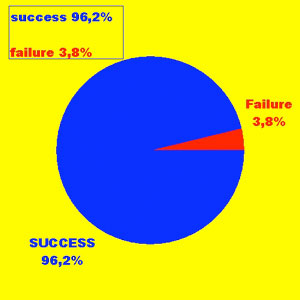
| RESULTS |
On 719 controlled patients scheduled for shoulder surgery, whih the only useof ENS there was a failure rate of 3,8%.
|
 |
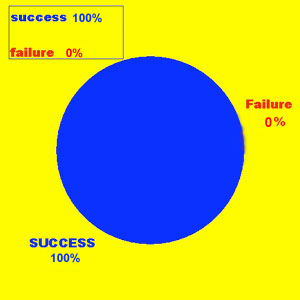
| |
After having applied the combined method U.S. + ENS, the 100% of succes rate has been reached.
|
 |
|
|
|
|
|
 |
|

